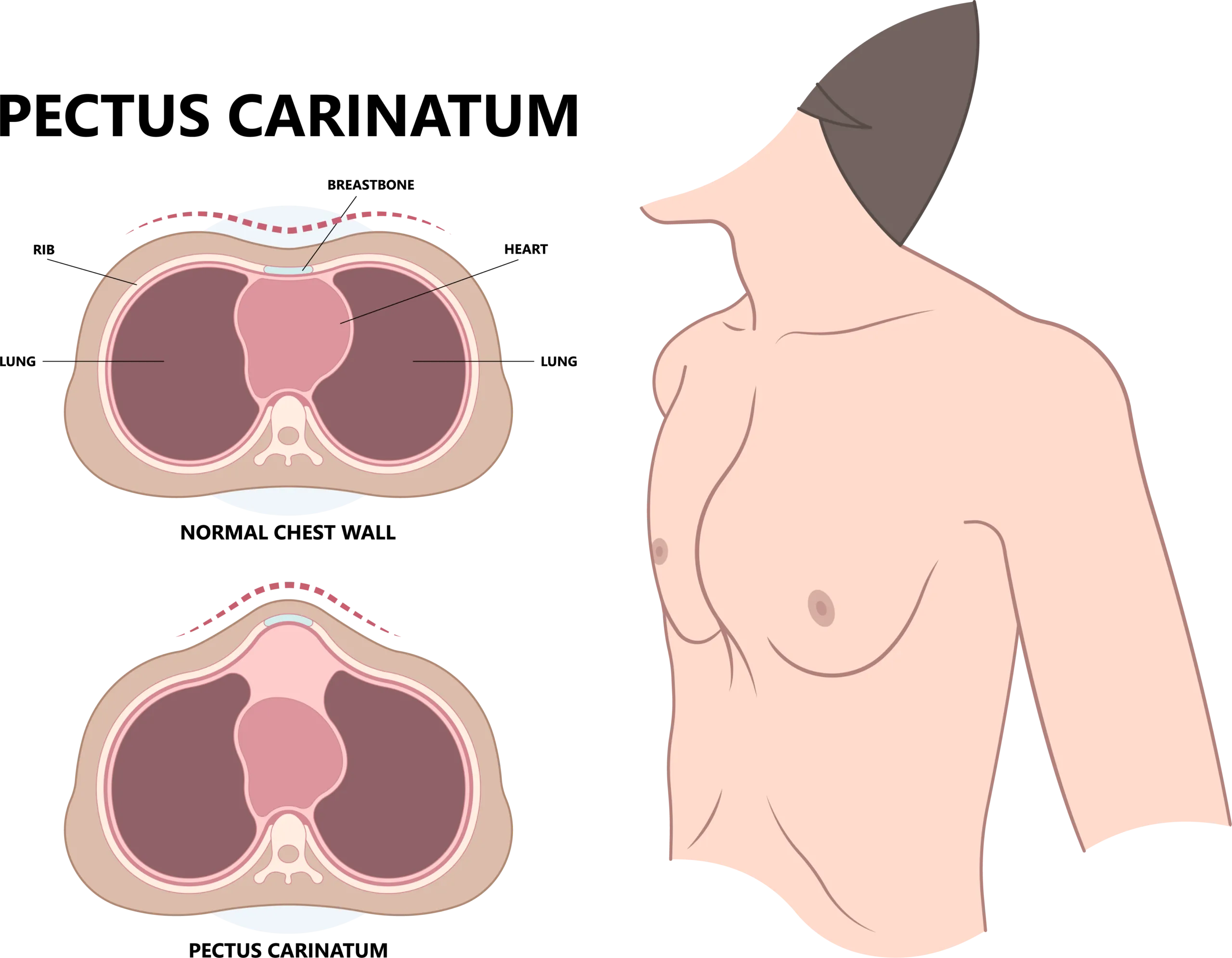
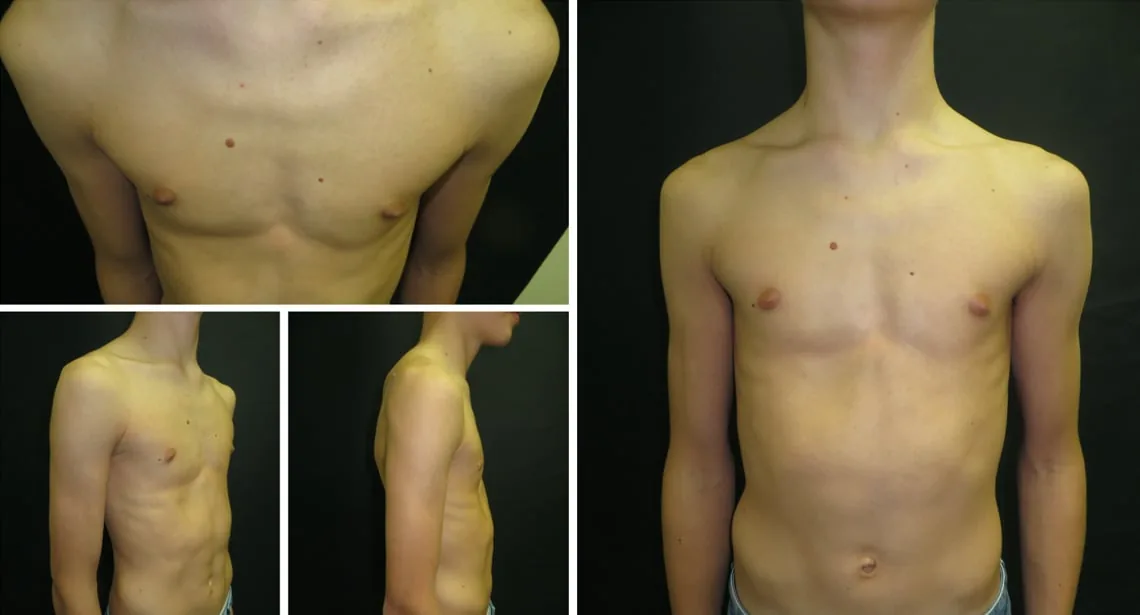
Physical Appearance

Physical Discomfort

Psychological Impact
"So even though we live about two and a half hours away, we feel that it's worthwhile to drive and see Dr. Abdullah because we had such a great experience with him and we trust his expertise in treating our son."
Jake McCoy 
"I actually found Dr. Abdullah after searching on YouTube. My experience with Dr. Abdullah has been amazing. He has really put myself at ease throughout this whole process, and I'm really happy with how everything's turned out."
Adam Patel